


A 68-year-old female with squamous cell carcinoma of the lower esophagus (cT3N0M0) developed an iatrogenic esophageal perforation following endoscopy, leading to mediastinitis.
The patient was initially managed conservatively. An attempt at endoscopic stenting was made; however, stent placement was not feasible as the distal lumen could not be identified endoscopically. By day 3, in view of worsening mediastinitis and a large perforation involving more than 50% of the esophageal circumference, a decision was made to proceed with surgical exploration.
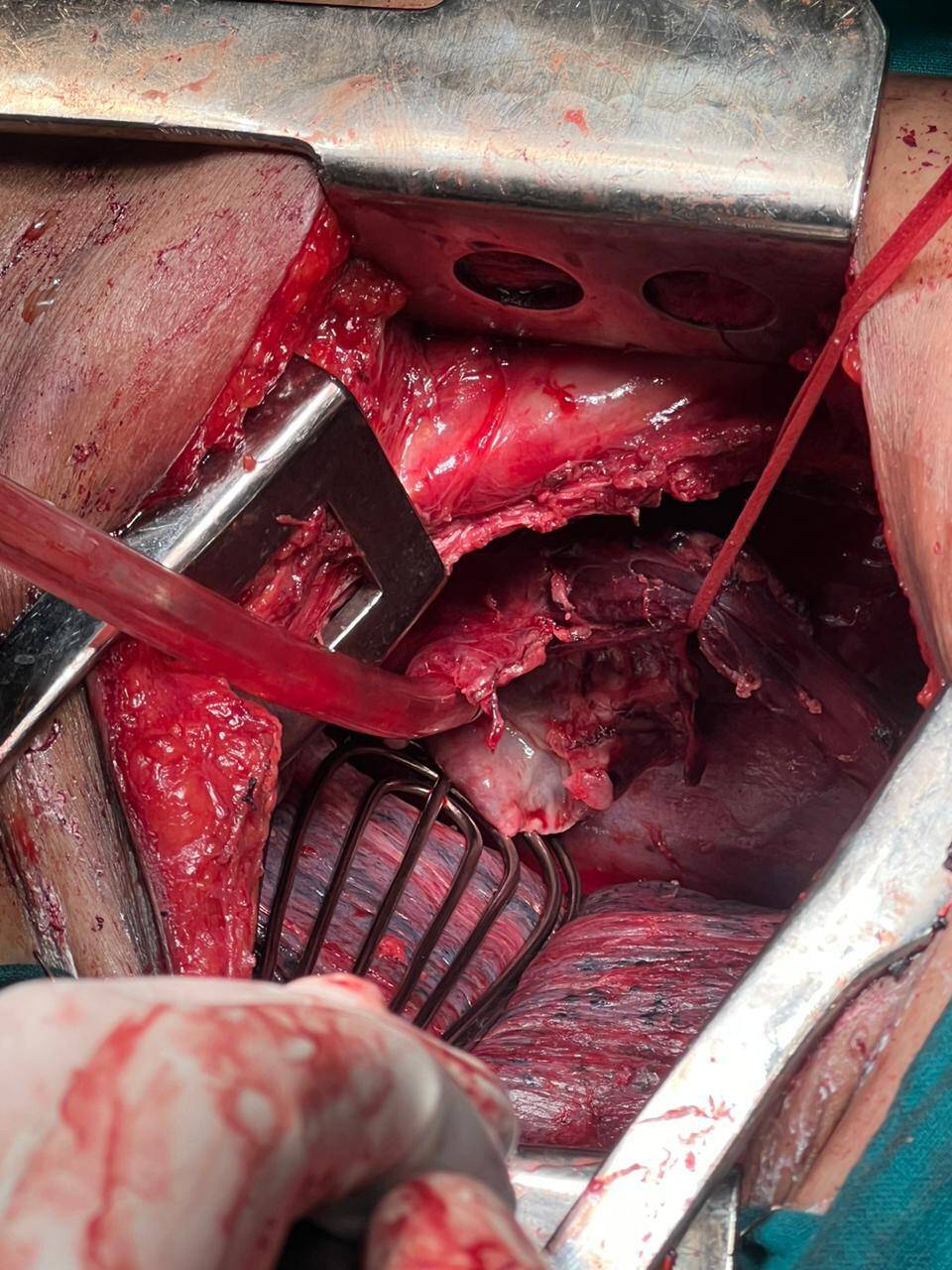
Given that the patient remained hemodynamically stable but showed progression of local sepsis, she underwent an emergency transthoracic esophagectomy with gastric conduit reconstruction. The procedure allowed definitive control of the source of contamination and restoration of gastrointestinal continuity.
The patient tolerated the surgery well. The postoperative course was complicated by pulmonary issues, which were managed effectively with intensive care support and dedicated pulmonary care.
With gradual recovery, the patient improved clinically and was discharged on postoperative day 12, tolerating oral intake and in stable condition.
This case highlights the importance of timely surgical intervention in esophageal perforation associated with malignancy, particularly when conservative and endoscopic measures are not feasible. In selected patients, emergency esophagectomy can be life-saving, offering both sepsis control and definitive oncologic management.